Oronasal Fistula
Oronasal Fistula Develops After Extraction of the Right Maxillary Canine
The patient’s lab work that morning was WNL. After administering pre-meds, an IV catheter was placed. The patient was induced, intubated, and placed in dorsal recumbency on an external heating source. General anesthesia was started, and monitoring devices were attached.
A complete oral exam including full mouth probing and charting was performed. Abnormals included a large right maxillary oronasal fistula, +3 mobility of 103, and two right maxillary retained premolar tooth roots and molar root protruding the gingiva.

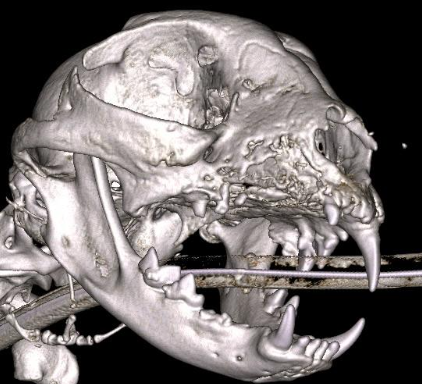
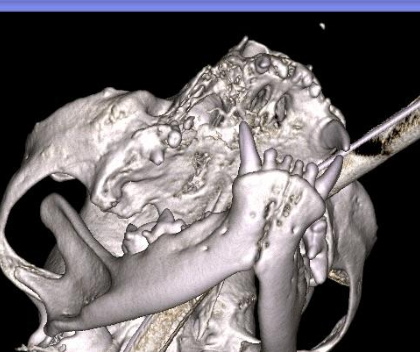
CBCT imaging was obtained and revealed five infected retained maxillary incisor tooth roots (lucency surrounded all 5 roots) and a root fracture of 103. Also retained were the mesial and distal roots of 107, palatal root of 108, and root of 109. The chronic oronasal fistula had caused severe maxillary bone, palatal bone, and right nasal turbinate destruction.
The patient’s healthy teeth were scaled and polished. Right and left maxillary nerve blocks using bupivacaine were performed. A large 3-corner flap was created. A mesial diverting vertical incision was started mesial to the oronasal fistula and extended to a few mm’s from the lip the lip margin. The flap coursed caudally along the maxilla to the distal aspect of 109 root. The flap was elevated off the maxilla and a few mm’s off the palatal bone. The oronasal fistula site was thoroughly debrided of dead, granulation, and unhealthy turbinate tissues. Surrounding dead bone was removed back to healthy bleeding bone. All unhealthy marginal tissue (alveolar and palatal) was removed. A mucoperiosteal incision was created the entire length of the flap to remove tension. The tension free flap was closed using 5-0 monocryl on a P3 needle.
An incision was made along the entire maxillary incisive region. All 5 retained incisor roots and 103 were extracted. Diseased tissue and bone were removed. Tissue edges were freshened, a mucoperiosteal releasing incision made, and tension free closure was performed.


Discussion
Unfortunately, cases like this are far too common. Proper extraction technique would have prevented the severe bone and soft tissue pathology and the need for a second much larger surgery. This cat showed no clinical signs for 20 months while the destruction was occurring. All extraction sites must be closed. All extraction sites must be closed without tension. Learning the different flap designs with tension release is not terribly difficult but it is also not intuitive. Taking an extraction course (or 2 or 3) is invaluable to hone your surgical skills, learn proper technique, and become faster and more efficient with your oral surgeries. Most cats and dogs do not show outward signs of oral discomfort. I highly recommend rechecking all your extraction patients two weeks following surgery. If this cat would have had a two week recheck the dehiscence would have been caught very early preventing two years of suffering and destruction.
Curt Ritchie DVM, DAVDC